Serosal surface appear dull, granular and erythematous
Cut section shows fecolith
Microscopy:
Sections show mucosa, submucosa, muscularis propria and serosal surface
Diagnostic: Neutrophilic infiltration up to muscularis propria
Chronic cholecystitis
Fig.
Fig.
Gross
Size: Shrunken gall bladder
Serosa: Smooth and appear dull
Cut section: Shows thickened wall, opaque and gray-white appearance
Lumen: Green-yellow velvety mucosa and stone
Microscopy:
Shows mucosa lined by columnar epithelium
Lamina propria shows lympho-plasmolytic infiltrate including lymphocytes, plasma cells and macrophages in mucosa
Marked subserosal fibrosis is noted
Tuberculosis, Lymph node
Microscopic features
Well-formed epithelioid granuloma composed of central caseous necrosis surrounded by epithelioid histiocytes
Multinucleated giant cells (Langhans giant cells)
Peripheral cuffing of granuloma by lymphocytes
Hyaline degeneration
Fig.
Fig.
Homogenous, glassy, eosinophilic appearance within cell or extracellular space.
It may also occur in vessel wall.
Hydropic degeneration
Melanin pigment
Fig.
Fig.
Histological features
Melanin is a brown pigment produced by melanocytes.
Melanin is made in melanosomes in melanocytes that are interspersed with basal cells of the epidermis.
Melanocytes interdigitate their cytoplasm with adjacent epidermal cells and transfer melanin granules to them.
Hemosiderin deposition (Pulmonary deposition)
Fig.
Microscopic features
Acute intra-alveolar hemorrhage is seen due to damage of capillaries
RBCs have come out of blood vessels into the alveoli.
Hemosiderin laden macrophages containing brown cytoplasmic hemosiderin granules from breakdown of RBCs may be seen it becomes chronic or long standing.
Epithelial cyst (Benign neoplasia)
Fig.
Fig.
Microscopic features:
Cyst lining composed of stratified squamous epithelium with a granular layer.
Cyst wall does not contain eccrine glands of hair follicles or sebaceous glands.
Cyst contents composed of abundant keratin flakes.
Foreign body giant cell reaction is frequently present in ruptured cysts.
Naevus (Benign neoplasm)
Fig.
Fig.
Microscopic features
The lesion is composed of melanocytes forming aggregates of nests at the dermo-epidermal junction (junctional naevus), which subsequently migrate to the underlying dermis (compound naevus). The older lesions may be entirely confined to the dermis (dermal naevus).
The melanocytes forming naevi are found to oral cells and have rounded or oval nuclei. The cytoplasm of naevus cells is homogeneous and contains abundant granular brown-black melanin pigment.
The pigment is more marked in the naevus cells in the lower epidermis and upper dermis, but the cells in the mid dermis and lower dermis hardly contain any pigment.
Adenocarcinoma, Stomach (Malignant neoplasia)
Fig.
Fig.
Microscopic features
Tubular and acinar pattern of growth is seen infiltrating the stomach wall
The tumor invades into the wall of the stomach for variable depth
The tumor cells show varying degree of anaplasia but are more often poorly differentiated with high degree of anaplasia
Squamous Cell Carcinoma (Malignant neoplasm)
Fig.
Gross (Lung)
This carcinoma usually arises centrally in the lung.
The neoplastic tissue is gray-white and firm to hard.
Areas of hemorrhage or necrosis.
Sometimes these necrotic foci cavitate.
Microscopic features
Tumor cells arranged in nests, cords, and single scattered.
Round to polygonal cells having abundant eosinophilic cytoplasm and round hyperchromatic nuclei.
Intercellular bridges.
Keratin pearls.
Basal Cell Carcinoma (Malignant neoplasm)
Fig.
Fig.
Microscopic features
Composed of nests, cords, islands of uniform basaloid cells growing deep into the dermis.
Peripheral palisading of tumor cells.
Retraction artifact from adjacent stroma.
Hyperplasia (BPH)
Fig.
Microscopic features
Both glands and stroma may be involved although hyperplasia of the former is usually more prominent.
Numerous crowded glands are present. There is still stroma between the glands.
The glands are larger than normal, with more complex infoldings but are still lined by a double layer of uniform columnar cells and basal cuboidal cells that show no atypia.
A rounded pink concentration, typical for corpora amylacea found in benign prostatic glands is present.
Coagulative necrosis (Infarct), Kidney
Fig.
Microscopic features:
The hallmark of coagulative necrosis kidney is that architectural outlines of glomeruli and tubules may be preserved through all cellular details are lost.
The margin of infarct shows inflammatory reaction, initially by polymorphonuclear cells but later macrophages, lymphocytes and fibrous tissue predominates.
Calcification
Microscopic findings
Histologically with the usual hematoxylin and eosin stain, calcium salts have a basophilic, amorphous granular, sometimes clumped appearance
They can be intracellular, extracellular, or in both locations
Thrombus
Fig.
Microscopic features
The internal elastic lamina is degenerated and is disrupted at the site of attachment of thrombus to the vessel wall
The residual lumen of the original artery is slit like and shows flowing blood.
The structure of thrombus shows lines of Zahn composed of layers of light-staining fibrin strands and platelets enmeshed in dark-staining red cells.
The underlying atheromatous plaque may be seen.
Organised thrombus shows ingrowth of granulation tissue at the base having spindle cells and capillary channels.
Congestion
Fig.
Microscopic features
Congestion is caused by venous obstrction.
There is enlargement of red pulp and diminished white pulp.
Dilated sinusoids filled with blood.
Areas of fibrosis are also seen.
Iron and Calcium containing fibrotic nodules (Gamma-gandy bodies) secondary to haemorrhage.
Abscess
Fig.
Hydatid cyst
Fig.
Laminated eosinophilic acellular membranous structure lined by inflammatory cells including lymphocytes and neutrophils.
Daughter cyst and booklets are not seen.
Hemangioma
Fig.
Microscopic features
Cavernous hemangioma has large dilated vascular channels filled with numerous red blood cells that extend to the underlying adipose tissue.
The vascular channels, which may vary in size and shape, are lined by flat endothelial cells.
A capillary hemangioma has smaller vascular channels.
Hemosiderin
Fig.
Fibrinoid necrosis
Fig.
Musculo-skeletal system
Lipoma
Fig.
Fig.
Fig.
Gross
Well circumscribed mass.
Yellowish globular tissue with thin fibrous septa on surface.
Greasy cut surface.
Microscopic features
Mature white adipose tissue.
Separated by fibrous septa.
Cytoplasmic vacuoles.
Liposarcoma
Fibrosarcoma
Benign fibrous histiocytoma
Malignant fibrous histiocytoma
Rhabdomyoma
Rhabdosarcoma
Leiomyoma
Fig.
Gross
Sharply circumscribed, discrete, round, firm gray-white tumors varying in size.
They can occur within the myometrium (intramural), just beneath the endometrium (submucosal), or beneath the serosa (subserosal).
The characteristic whorled pattern of smooth muscle cells on the cut section makes these lesions readily identifiable.
Microscopic features
Interlacing bundles of uniform spindle cells.
Mitoses are not seen.
The cytoplasm of smooth muscle fibers is more pink, and their nuclei are short, plump, and fusiform.
Larger leiomyomas may have central softening with hemorrhage.
Associated with hyalinization.
Leiomyosarcoma
Fig.
Leprosy
Fig.
Lepromatous leprosy
Microscopic features
The dermis contains large aggregates of lipid-laden foamy macrophages known as lepra cells.
The dermal infiltrate of lepra cells characteristically does not encroach upon the basal layer of epidermis leaving uninvolved (Clear zone) subepidermal dermis.
The overlying epidermis is thin and flat.
With fite-faraco stain, lepra cells are crowded with acid fast lepra bacilli.
Tuberculoid leprosy
Microscopic features
The dermis shows granulomas which closely resemble hard tubercles i.e, they consist of epitheloid cells, langhans giant cells and a few lmyphocytes at the periphery but generally little or no caseation necrosis.
The granulomas erode the basal layer of the epidermis, i.e., there is no clear zone.
The lesions of tuberculoid leprosy have predilection for dermal nerves which may be destroyed and infiltrated by epitheliod cells and lymphocytes.
With fite-faraco stain, lepra bacilli are almost never found (paucibacillary leprosy).
Osteosarcoma
Fig.
Fig.
Fig.
Fig.
Gross features
They are bulky, grey white tumors arising from the medullary cavity.
They contain areas of hemorrhage.
Microscopic features
Tumor cells demonstrate pleomorphism.
Tumor cells have large hyperchromatic nuclei with occasional tumor giant cells.
Abundant mitosis are seen in the tumor.
New bone formation by tumor cells.
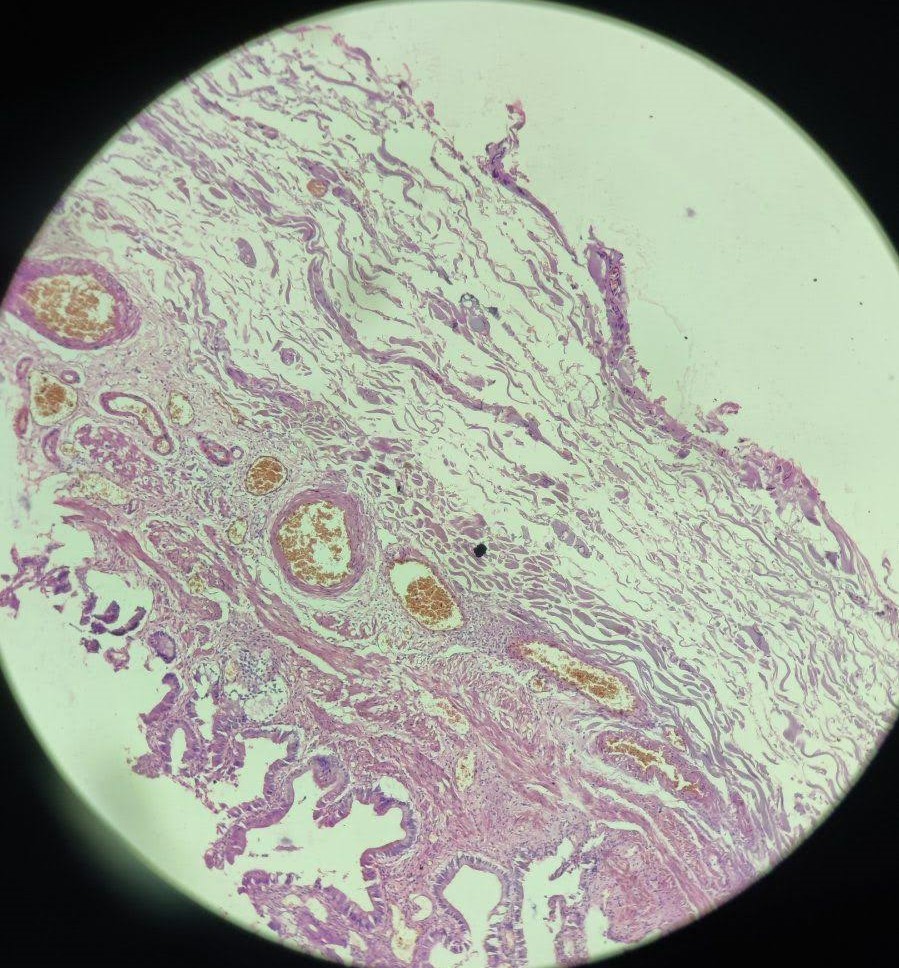
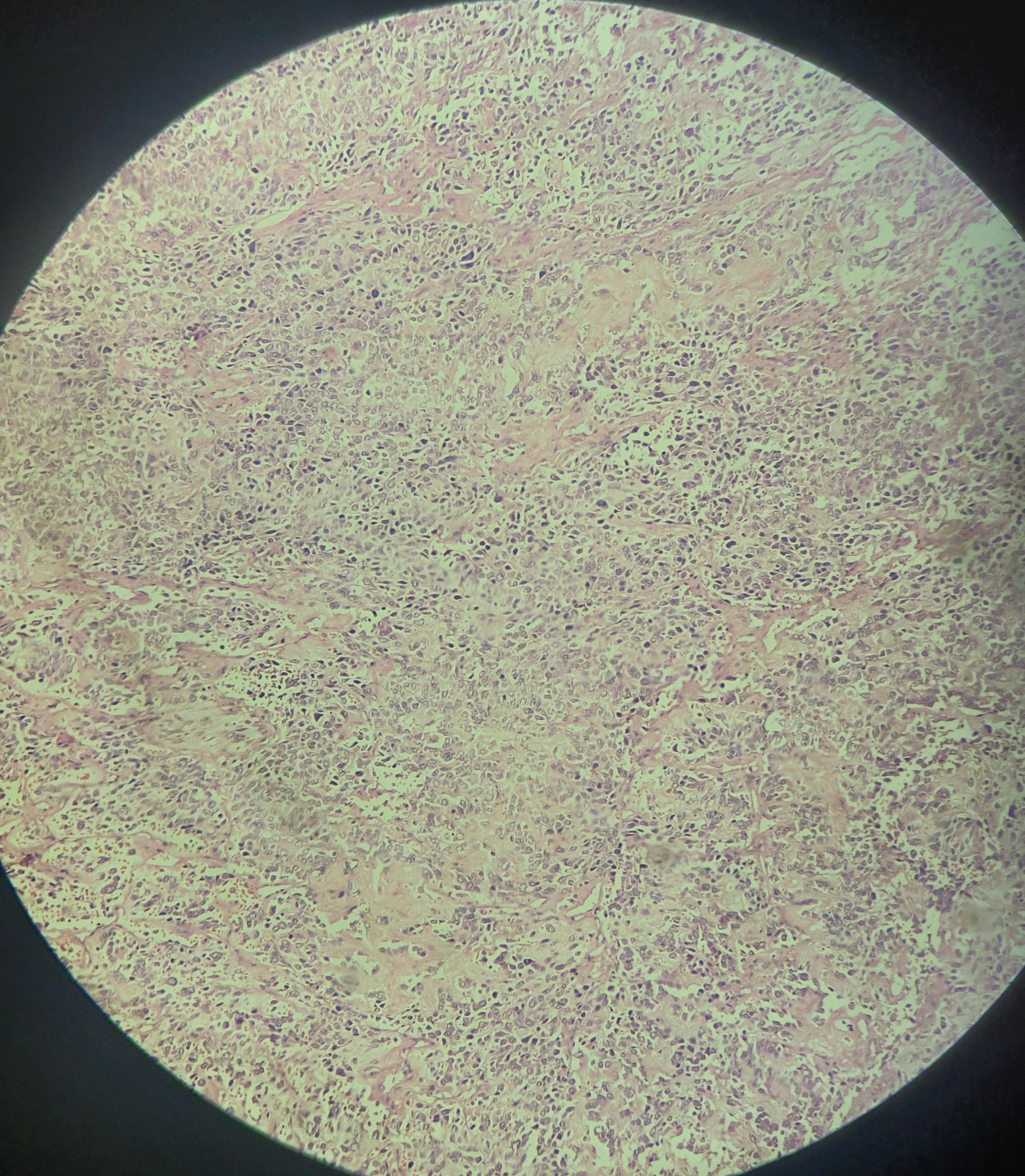
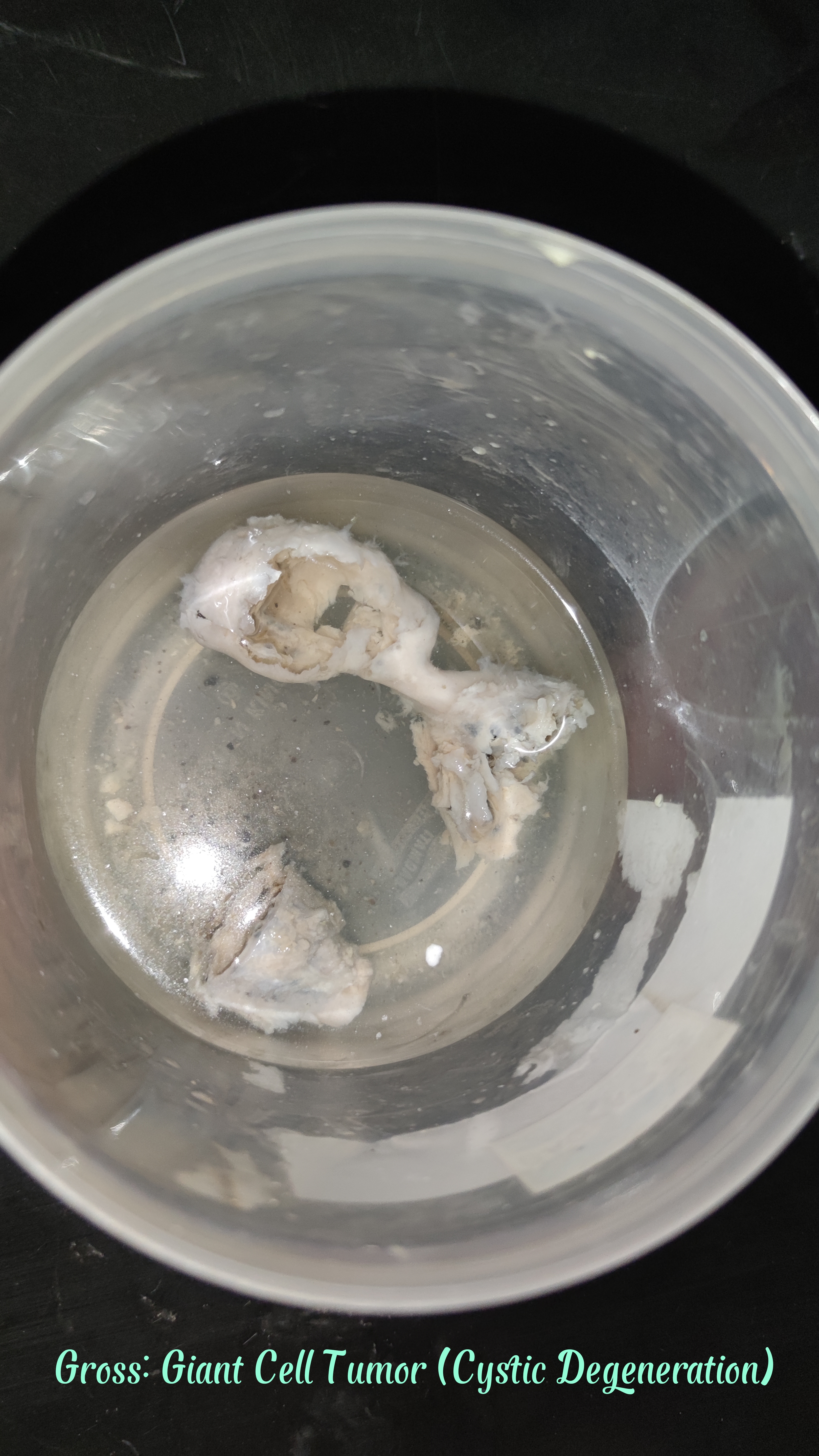
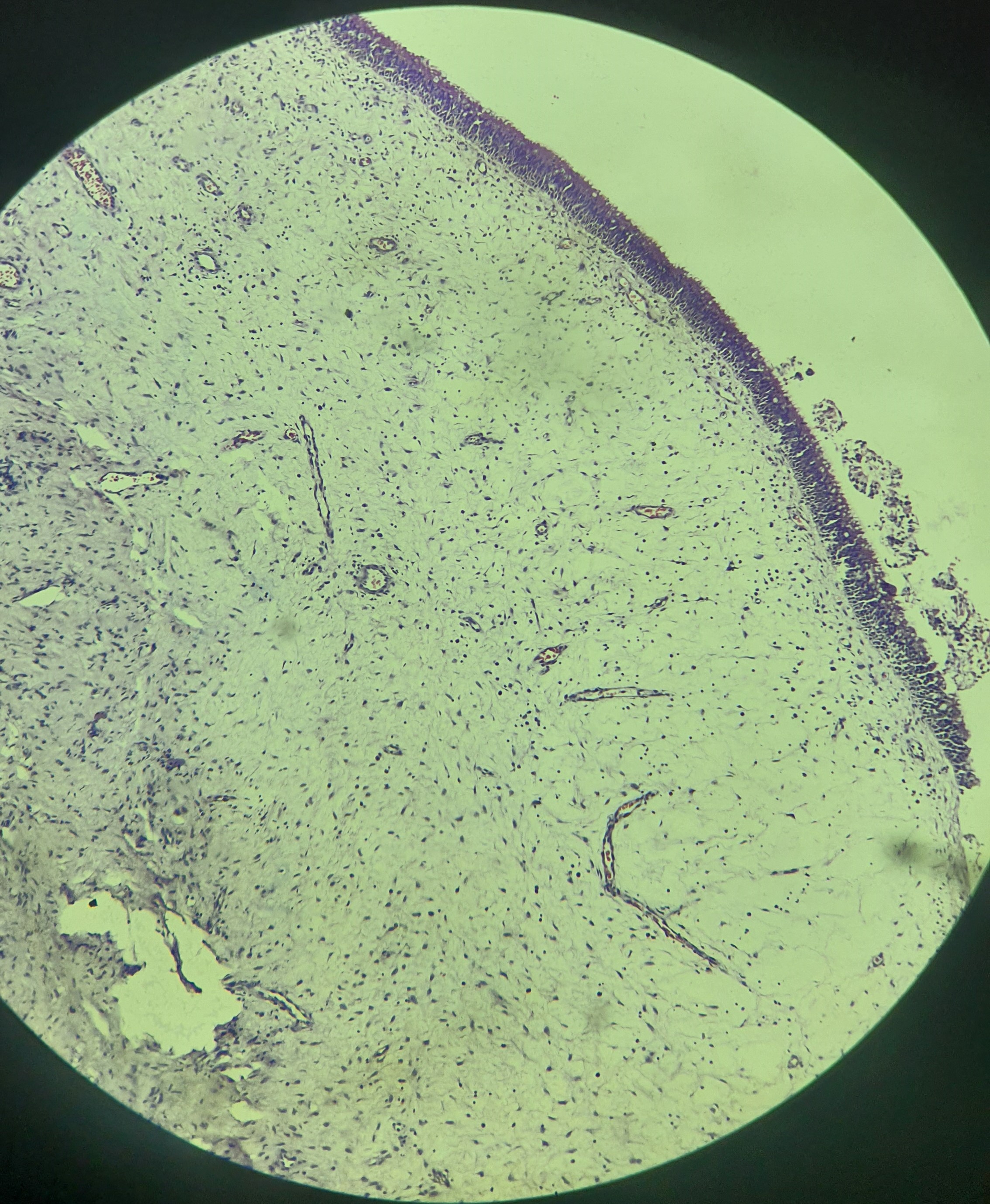
Giant Cell Tumor
Fig.
Fig.
Fig.
Fig.
Gross features
Tumour is eccentrically located in the epiphyseal end of a long bone.
Cut surface of the tumor is hemorrhagic, necrotic and honey combed.
Surrounding cortex is thinned out.
Microscopic features
Numerous osteoclast like giant cells with 100 or more nuclei.
Large mononuclear cells.
Vascular stroma, necrosis and mitoses are seen.
Ewing sarcoma
Fig.
Gross
Arising in the medullary cavity, tumor usually invades the cortex, periosteum and soft tissue.
The tumor is soft tan-white and frequently contains area of hemorrhage and necrosis.
Microscopic features
Tumor is composed of small rounded cells with scanty cytoplasm.
Homa-wright rosette are present which consists of rounded cell clusters with a central fibrillary core.
Fibrous septa are also seen separating the tumor cells.
Nervous system
Meningitis
Tuberculoma
Astrocytoma
Fig.
Glioblastoma multiforme
Fig.
Fig.
Microscopic features
Hypercellular with increased nuclear atypia
Pseudopalisaidng necrosis (Tumor Cells around necrosis)
Fibrillary background
Oligodendroglioma
Fig.
Fig.
Tumor cells in sheets with spherical nuclei containing finely granular chromatin surrounded by a clear halo of vacuolated cytoplasm
Network of anastomosing capillaries, resembling "Chicken wire"
Calcification, mitotic figures and necrosis
Tumor cells that infiltrate the cerebral cortex often collect around neurons (perineuronal satelitosis).
Ependymoma
Meningioma
Fig.
Neurofibroma
Fig.
Microscopic features
Neurofibroma consists of bundles of wavy elongated spindle cells with small dark oblong nuclei and a lot of intervening collagen.
Schwannoma
Fig.
Microscopic features
Spindle-shaped tumor cells.
Hypercellular areas (Antoni A) and hypocellular areas (Antoni B).
Verrucay bodies.
Retinoblastoma
Fig.
Fig.
Gross features:
Creamy white mass with yellow necrotic areas.
Chalky areas of calcification.
Grows inward (endophytic) or outward (exophytic).
Microscopic features
Tumor composed of small round cells with hyperchromatic nuclei.