Mucinous secretion seen and appear gelatinous and glairy.
Microscopic:
Tumor cells are arranged in tubules and glands.
These tumor cells have scant amount of eosinophilic cytoplasm, round to ovoid nuclei, opened up chromatin and small nucleoli.
Cardiovascular System
Microcytic Hypochromic Anaemia
Fig.
RBCs size is smaller than the nucleus of mature lymphocytes.
Central pallor more than one third.
Seen in iron deficiency anaemia, thalassemia, anaemia of chronic disease, sideroblastic anaemia.
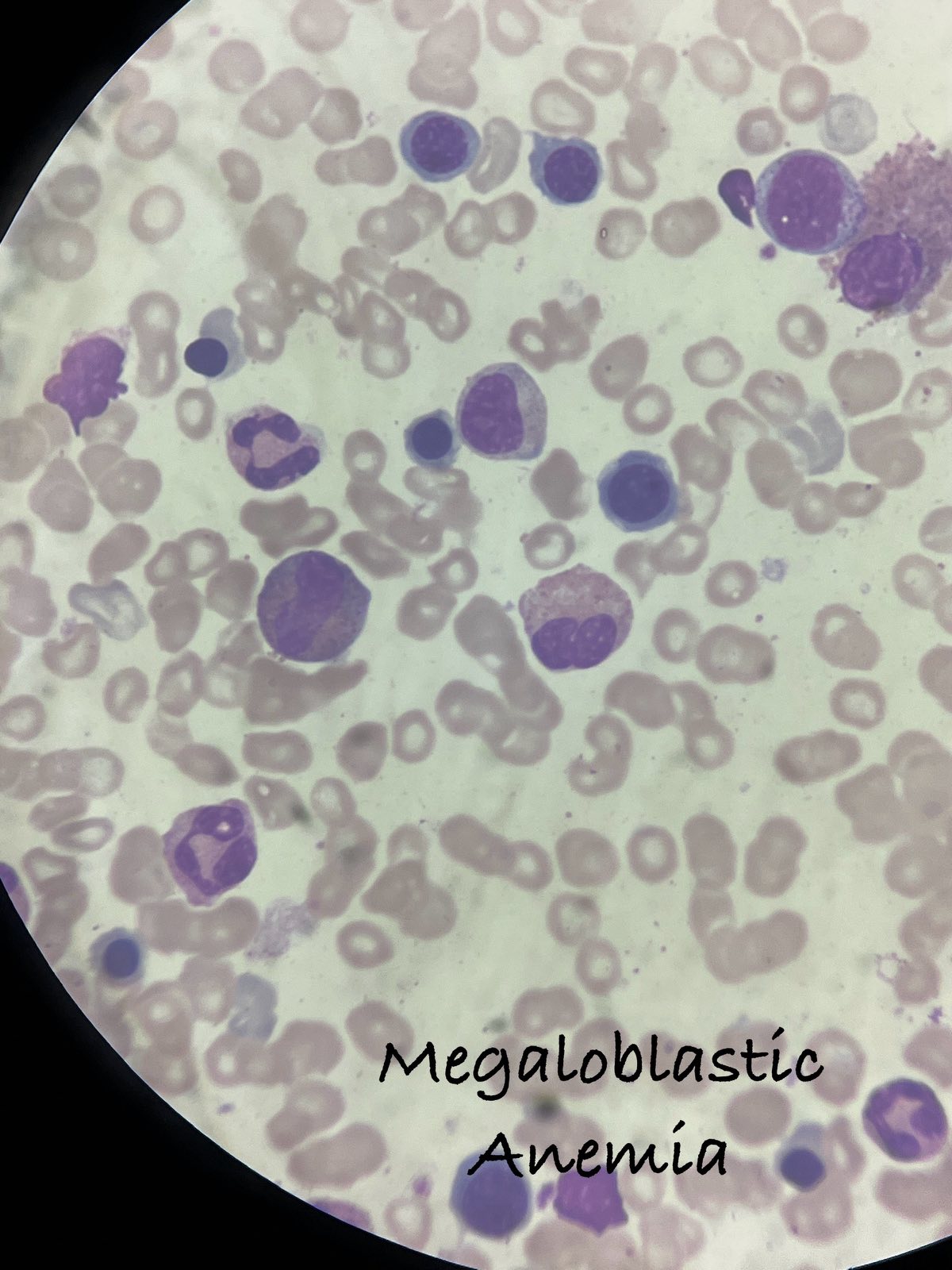
Macrocytic Anaemia
Fig.
RBC size larger than the nucleus of mature lymphocytes.
Hypersegmented neutrophils are an associated finding.
Seen in vitamin B12 and folate deficiency alcoholic liver disease.
Megaloblastic Anaemia
Fig.
Fig.
Bone marrow findings
Hypercellular marrow.
Erythroid hyperplasia with dyserythropoietic changes in the form of sieve like chromatin and binucleation.
Increased granulopoiesis with giant metamyelocytes may be seen.
Megakaryocytes may also show hyperlobulation.
Acute Myeloid Leukemia (AML)
Fig.
Fig.
Fig.
Leukocytosis.
Atypical cells/ Blasts with increased size (>20%).
Moderate amount of cytoplasm.
Increased N:C ratio.
2-3 prominent nucleoli.
Auer rods (needle like azurophilic granules) are seen.
Acute Lymphoblastic Leukemia (ALL)
Fig.
Fig.
Fig.
Leukocytosis.
Presence of lymphoblast >/= 20%.
Lymphoblasts having high N:C ratio and scant, agranular cytoplasm.
Nuclei have coarse nuclear chromatin and inconspicuous to occassional prominent nucleoli.
More common in children.
Chronic Myeloid Leukemia (CML)
Fig.
Fig.
Fig.
Leukocytosis.
Increase in myeloid lineage of cells band forms, metamyelocytes, myelocytes, neutrophils, eosinophils, basophils.
Blasts are variable in number according to the 3 different phases (Chronic, accelerated, blast crisis), usually less than 10%.
Increased platelets.
Chronic Lymphocytic Leukemia (CLL)
Fig.
Fig.
Fig.
Leukocytosis.
Increased small round lymphocytes having scant cytoplasm.
Presence of smudge cells.
Occurs in adults
Non-Hodgkins Lymphoma
Fig.
Fig.
Loss of normal architecture of lymphocytes.
Presence of monotonous population of lymphoid cells.
These cells are medium to large with round nucleus, coarse chromatin, prominent nucleoli, and scant cytoplasm.
Mitosis may be frequent.
Reactive Lymphadenopathy
Enlarged follicles, varying in size and shape with prominent germinal center.
Prominent sinuses may be seen.
Myocardial Infarction
Fig.
Coagulative necrosis of cardiac muscles.
Neutrophilic infiltrates are seen in between muscle bundles.
Atherosclerosis
Plaque obstructing the lumen.
Overlying fibrous cap.
Contains macrophages, lymphocytes, lipids deposited in tunica media.
Well-formed necrotic core.
Aneurysm
Fig.
Destruction and thinning of tunica media along with myxoid changes.
Replacement of tunica media by hyalinized connective tissue.
Fragmentation of elastin in artery wall.
In case of dissecting aneurysm, theres is a tear in intima, interna and blood trickles in between the layers of blood vessel wall.
Inflammatory reaction composed mostly of lymphocytes and macrophages is noted.
Atherosclerosis and hypertension are most common cause.
Gastrointestinal System
Acute Appendicitis
Fig. Acute appendicitis
Gross:
Appendix appears swollen.
Serosa is hyperaemic and coated with fibrino purulent exudate and appears dull, granular and erythematous.
The mucosa is ulcerated and sloughed.
Cut section shows fecolith.
Microscopy:
Most important diagnositc feature is neutrophilic infiltration of the muscularis propria.
Mucosa is sloughed and blood vessels in the wall are thrombosed.
Periappenddiceal inflammation is seen in advanced cases.
Sections shows mucosa, submucosa, muscularis propria and serosal surface.
Pleomorphic Adenoma
Usually well demarcated and encapsulated, rarely exceeding 6cm in greatest dimension.
Typically has 3 components:
i. Epithelial (ductal) components: Cuboidal to columnar epithelial cells forming the inner layer of acini and tubules.
ii. Myoepithelial cells as the outer layer of acini, tubules or scattered within the myxoid stroma in strands or sheets of cells.
iii. Stromal component: Consists of loose myxoid tissue containing islands of cartilage and rarely foci of bone.
Chronic Sialadenitis
Maintained lobular architecture.
Varying degrees of acinar destruction, fibrosis and chronic inflammation with lymphoid aggregates containing prominent germinal centers.
Ducts may undergo squamous and mucous metaplasia.
Can be caused by trauma, bacterial or viral (mumps) infection and autoimmune disease (Sjogren's syndrome).
Adenoid Cystic Carcinoma
Tumor composed of ductal cells having hyperchromatic, angulated compact nuclei and scant cytoplasm and myoepithelial cells with flattened nuclei.
Tumor cells arranged in tubular, solid or cribiform pattern.
Spaces between tumor cells are filled with hyaline material which represents excess basement membrane material.
Chronic Cholecystitis
Fig.
Gross:
Size: Shrunken gall bladder.
Serosa: Smooth and appear dull.
Cut section: Shows thickened wall, opaque and gray-white appearance.
Lumen: Green-yellow, mucoid bile and stone.
Microscopy
Shows mucosa lined by columnar epithelium.
Lamina propria shows lympho-plasmocytic infiltrate including lymphocytes, plasma cells and macrophages in mucosa.
Marked subserosal fibrosis is noted.
Chronic Active Gastritis
Gastric mucosa lined by columnar epithelial cells.
Lamina propria shows lymphocytes, plasma cells and neutrophils.
There is infiltration of pits or glands by neutrophils.
Stomach Carcinoma
Gross:
Polypoidal friable mass.
Grey white in color.
Microscopy:
Tumor cells are arranged in glands and tubules.
These tumor cells are pleomorphic with high N:C ratio.
Apical mucin may ne seen.
Cirrhosis
Fig.
Regenerative nodules surrounded by bridging fibrous septa.
Diffuse disruption in architecture of the liver.
Colonic Adenocarcinoma
Gross:
Polypoidal mass.
Friable, grey white in color.
Microscopy:
Tumor cells arranged in glands and tubules.
Glands are lined by stratified columnar epithelium.
Tumor cells have round to oval nuclei, vesicular chromatin and prominent nucleoli.
Necrosis can be seen.
Hepatocellular Carcinoma
Fig.
Fig.
Fig.
Loss of tissue architecture with tumor cells arranged mostly in trabecular and pseudoglandular pattern.
Moderately pleomorphic tumor cells with moderate amount of granular eosinophilic cytoplasm, oval nuclei and prominent nucleoli.
Pancreatic Carcinoma (Gross)
Gross:
Very firm, stellate, gray-whtie, poorly delinated and firm masses.
About 60% in the head, 15% in body and 5% in tail.
It can obstruct the common bile duct.
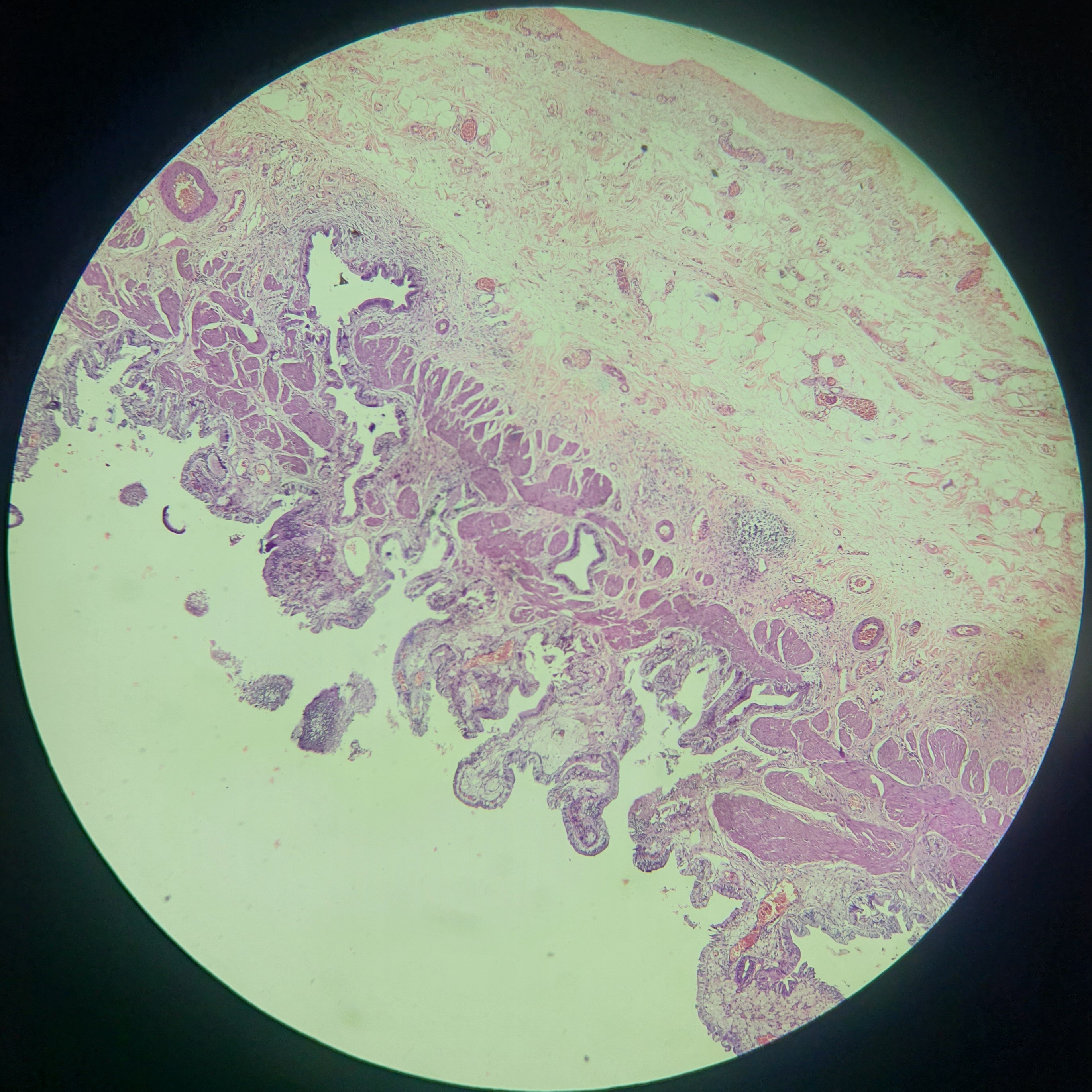
Juvenile Polyp
Fig.
Microscopic:
Dilated glands filled with mucin and inflammatory debris.
Lamina propria expanded by mixed inflammatory infiltrates.
The muscularis mucosa may be normal or attenuated.
Surface erosion and cystically dilated crypts.
Tubulovillous Adenoma
Fig.
Microscopic:
Glandular or villous architecture with dysplastic epithelium.
Histologically, the hallmark of epithelial dysplasia is nuclear hyperchromasia, elongation and stratification.
Reduction in the number of goblet cells.
Prominent nucleoli and eosinophilic cytoplasm may be seen.
Renal System
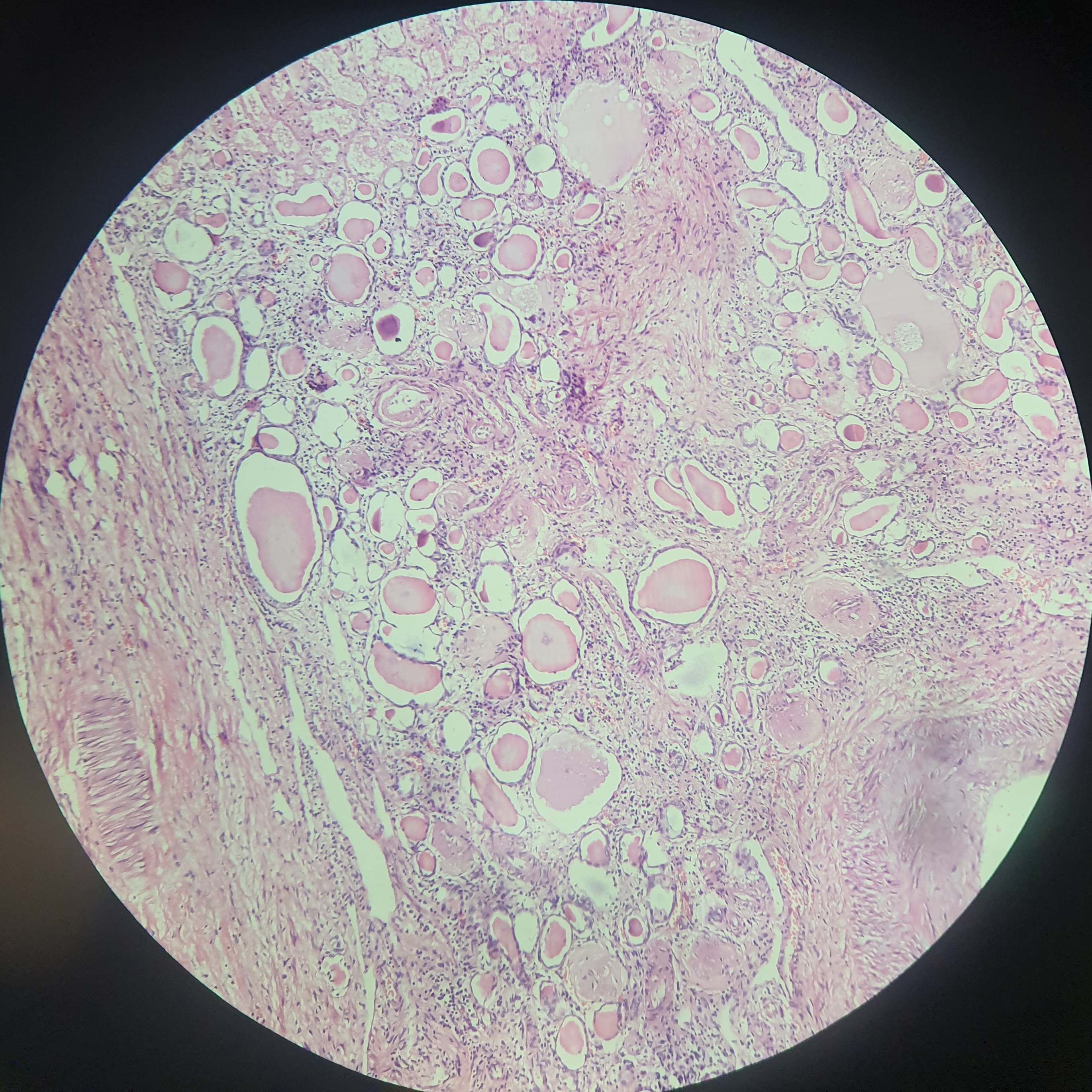
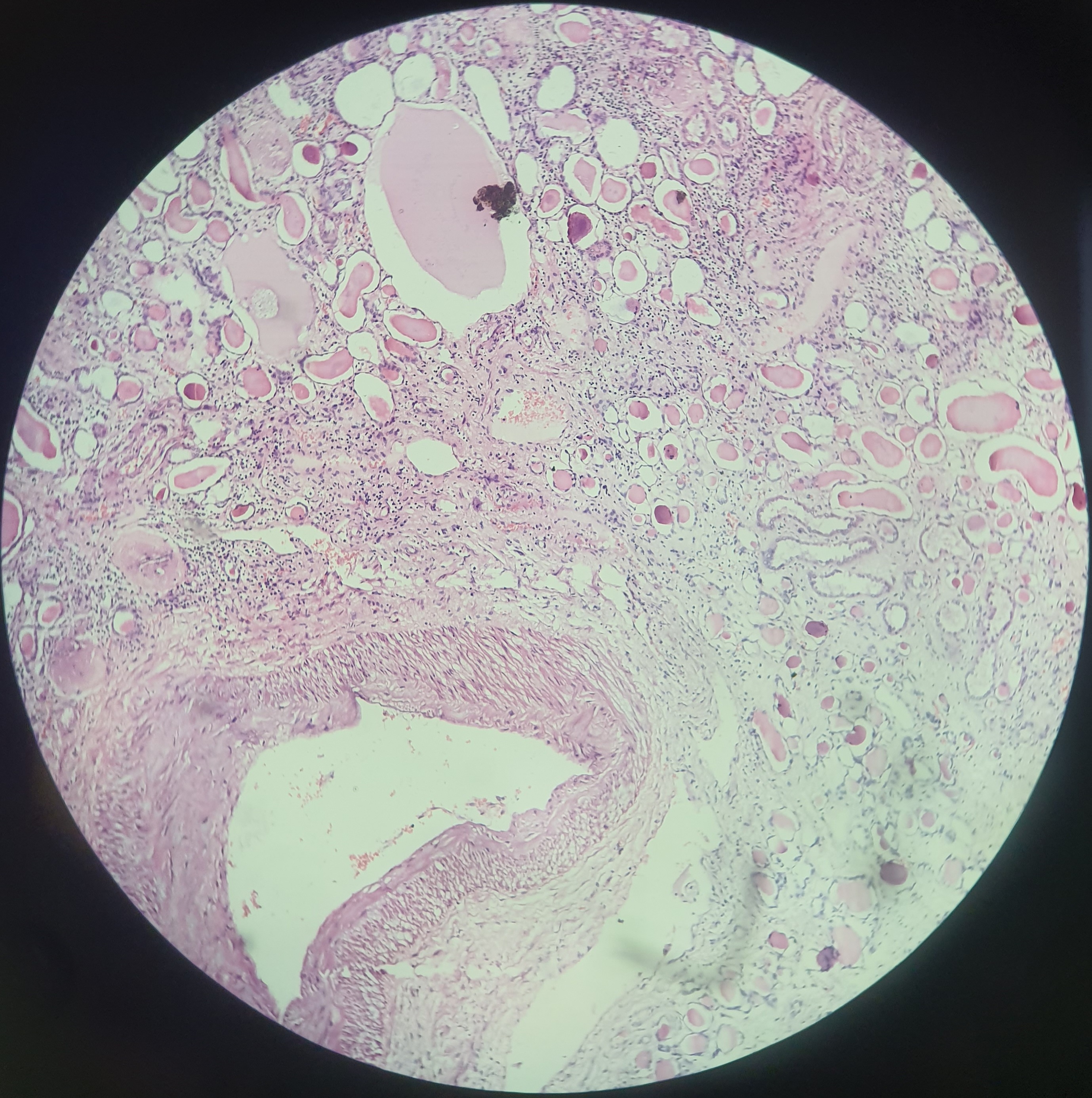
Chronic Pyelonephritis
Fig.
Fig.
Fig.
Microscopic:
Uneven interstitial fibrosis and an inflammatory infiltrate of lymphocytes, plasma cells and occassionally neutrophils.
Dilation or contraction of tubules, with atrophy of the epithelial lining (Tubular atrophy).
Tubular thyroidizaiton (filled with colloid casts): Many of the dilated tubules contain pink to blue, glassy-appearing PAS-positive casts, known as colloid cast, that suggest the appearance of thyroid tissue.
Clear Cell Renal Cell Carcinoma (ccRCC)
Fig.
Microscopic:
Tumor cells arranged in tubules, cords or sheets.
Round to polygonal cells having vacuolated (lipid laden) to clear cytoplasm demarcated only by their cell membranes. The nuclei are usually small and round.
Characteristic network of small, thin walled, "chicken wire" vasculature.
Gross:
Specimen: Kidney
There is a mass measuring variable sizeds that distort the renal outline.
Cut surface: Yellow to gray-white, with prominent areas of cystic softening of or hemorrhage.
Wilms Tumor
Fig.
Microscopy:
Typically consists of 3 components: Blastemal, Epithelial and stromal.
Blastemal component: Consist of sheets of small blue cells having small regular nuclei and small nucleoli.
Epithelila component: Usually takes the form of abortive tubules or glomeruli.
Stromal component: Usually fibrocytic or myxoid in nature.
Hydronephrosis
Gross:
Massively enlarged kidney.
Greatly distended pelvicalyceal system.
Thin cortical rim due to atrophy by renal cell carcinoma (clear cell).
Urothelial Carcinoma
Fig.
Increased thickness and fused and branching papillae which show disorderly arrangement.
Tumor cells show nuclear enlargement, moderate to marked variation in nuclear size, shape, hyperchromatism.
Multiple prominent nucleoli.
Mitosis are frequent and atypical.
Reproductive System
Seminoma
Fig.
Composed of sheets of uniform cells divided into poorly demarcated lobules by delicate septa of fibrous tissues containing moderate amount of lymphocytes.
Seminoma cells are large, round to polyhedral and have a distinct cell membrane, a clear or watery appearing cytoplasm containing varying amount of glycogen.
Cells with large central nucleus with 2 or more prominent nucleoli.
Prostatic Carcinoma
Neoplastic glands are usually smaller than benign glands.
In contrast to benign glands, prostate cancer glands are more crowded, and lack branching and papillary infoldings.
Glands are lined by a single uniform layer of cuboidal or low columnar cells.
Outer basal cell layer, which is seen in benign glands is absent.
Cytoplasm ranges from pale-clear to a distinctive amphophilic appearance.
Nucleoli are large and may contain one or more large nucleoli.
Benign Prostatic Hyperplasia (BPH)
The hallmark of BPH is nodularity, the composition of which ranges from stromal fibromuscular nodules to fibro epithelial nodules with a glandular predominance.
Glandular proliferation takes the form of aggregation of small to large to cystically dilated glands lined by two layers, an inner columnar and an outer cuboidal or flattened epithelium.
Glands also show intra-acinar papillary infolding with delicate fibro-vascular core.
Foci of lymphocytic aggregates, small areas of infarction, corpora amylacea and foci of squamous-metaplasia are found.
Serous Cystadenoma
Gross
Usually 3-10 cm (but can be upto 30 cm), oval to round, smooth glistening surface.
Contains usually clear to pale yellow cyst fluid.
Microscopy
Cyst wall lined by cuboidal to columar lining with cilia.
Underlying stroma shows spindle fibroblasts.
Papillae are seen.
Serous Cystadenocarcinoma
Microscopy:
Infiltrating tumor arranged in sheets, nests and fused papillae.
These tumor cells have moderate amoun of eosinophilic cytoplasm, round to oval nuclei, coarse to vesicular nuclear chromatin and prominent nucleoli.
These tumor cells exhibit moderate to marked degree of nuclear pleomorphism.
Product of Conception
Microscopy
Chorionic villi lined by trophoblastic cells and syncytiotrophoblastic cells.
Decidualised stroma, fibrinoid material and blood clots.
Hydropic changes or atypical cells are not seen.
Tubal Ectopic
Microscopic:
Sections examined from fallopian tube shows presence of chorionic villi or extravilllous trophoblasts.
Extensive hemorrhage and fibrin deposits.
No hydropic degeneration of villi and atypical cells are seen.
Secretory Endometrius
Glands are tortous.
Subnuclear and supranuclear vacuolation can be seen.
Stroma is edematous.
Mucinous Cystadenoma
Microscopy:
Cyst and glands are lined by a single layer of mucin containing columnar cells.
Underlying stroma is cellular and shows fibroblasts.
Focal papillae are seen.
Mucinous Cystadenocarcinoma
Infiltrative glands lined by cells having high N:C ratio and vesicular chromatin and prominent nucleoli.
Surrounding stroma is desmoplastic.
Mitosis is frequent.
Hydatidiform Mole
Complete male microscopy:
Most of chorionic villi are enlarged, scalloped in shape with central cavitation (cisterns).
Villi are covered by extensive trophoblastic proliferatioon that involve the entire circumference of the villi.
Partial male microscopy:
Some of the villi are enlarged and edematous.
Trophoblastic hyperplasia is focal and less marked.
Vasculature and nucleated RBCs are seen.
Leiomyoma (Gross)
Gross
Well defined, circumscribed globular mass.
Whitish in color.
Cut section shows white homogenous area showing whorling pattern.
Ovarian Teratoma
Gross:
Smooth unilocular cyst, generally < 10 cm.
Cut section shows a thin wall lined by opaque, gray-white, wrinkled epidermis and may contain hair, teeth, cartilage, bone or sebaceous material.
Raised protuberance in cyst wall (Rokitansky nodule).
Cervical Carcinoma (SCC Cervix)
Microscopic features:
Tumor cells arranged in nests, cords and singly scattered pattern.
Round to polygonal cells having abundant eosinophilic cytoplasm and round hyperchromatic nuclei.
Intercellular bridges.
Keratin pearls.
Benign Endocervical Polyp
Microscopy:
Polypoidal tissue lined by endocervical (and partly by SSE).
Underlying stroma shows dilated endocervical glands and chronic inflammatory infiltrates along with proliferating blood vessels.
Endometrial endometriod carcinoma
Tumor cell are arranged in back to back glands lacking intervening stroma.
Moderately differentiated show well-formed glands mixed with areas composed of solid sheets of cells, (<50%) and poorly differentiated characterised by >50% solid growth pattern.
These cells have enlarged round nuclei with large nucleoli and eosinophilic cytoplasm.
Loss of polarity, desmoplastic reaction and squamous differentiation may be seen.
Resembles proliferative type endometrium.
Fibroadenoma
Gross:
Firm, well circumscribed, ovoid mass with bosselated surface, lobulations bulge above the cut surface.
Microscopic:
Proliferation of both glandular and stromal elements.
Glandular component arranged in intracanalicular and pericanalicular pattern.
Glands are lined by epithelial cells and surrounded by myoepithelial cells.
Myxoid stroma is noted.
Leiomyoma
Microscopic:
Well circumscibed mass.
Fascicles and bundles of smooth muscle cells.
These cells are spindle in shape with elongated in cigar shaped nuclei and eosinophilic cytoplasm.
Mitosis, necrosis and atypia are not seen.
Choriocarcinoma
Microscopic
Solid sheets of atypical syncytiotrophoblast, cytotrophoblast and intermediate trophoblast.
Absence of chorionic villi.
Background show necrosis and hemorrhage.
Invasive Breast Carcinoma, NST
Microscopic:
Tumor cells are arranged in sheets, nests, cords, tubules and singly scattered cells.
These tumor cells have moderate amount of cytoplasm round to oval nuclei with coarse nuclear chromatin.
No myoepithelial cell lining.
Mature Ovarian Teratoma
Microscopic
Cyst lined by stratified squamous epithelium.
Cyst wall shows pilosebaceous unit, hair shaft, blood vessels adipocytes.