▢ Localising lesions in the central nervous system:
INVESTIGATION OF NEUROLOGICAL DISEASE
▢ Neuroimaging:
▢ Neurophysiological testing:
PRESENTING PROBLEMS IN NEUROLOGICAL DISEASE
▢ Headache and facial pain:
▢ Dizziness, blackouts and 'funny turns':
▢ Status epilepticus:
▢ Coma:
▢ Delirium:
▢ Amnesia:
▢ Weakness:
▢ Sensory disturbance:
▢ Abnormal movements:
▢ Abnormal perception:
▢ Altered balance and vertigo:
▢ Abnormal gait:
▢ Abnormal speech and language:
▢ Disturbance of smell:
▢ Visual disturbance and ocular abnormalities:
▢ Hearing disturbance:
▢ Bulbar symptoms – dysphagia and dysarthria:
▢ Bladder, bowel and sexual disturbance:
▢ Personality change:
▢ Sleep disturbance:
▢ Psychiatric disorders:
FUNCTIONAL SYMPTOMS
HEADACHE SYNDROMES
EPILEPSY
VESTIBULAR DISORDERS
DISORDERS OF SLEEP
▢ Excessive daytime sleepiness (hypersomnolence):
▢ Parasomnias:
NEURO-INFLAMMATORY DISEASES
PARANEOPLASTIC NEUROLOGICAL DISORDERS
NEURODEGENERATIVE DISEASES
▢ Movement disorders:
▢ Ataxias:
▢ Tremor disorders:
▢ Dystonia:
▢ Hemifacial spasm:
▢ Motor neuron disease:
▢ Spinal muscular atrophy:
INFECTIONS OF THE NERVOUS SYSTEM
▢ Meningitis:
▢ Parenchymal viral infections:
▢ Parenchymal bacterial infections:
▢ Diseases caused by bacterial toxins:
▢ Prion diseases:
INTRACRANIAL MASS LESIONS AND RAISED INTRACRANIAL PRESSURE
▢ Raised intracranial pressure:
▢ Brain tumours:
▢ Paraneoplastic neurological disease:
▢ Hydrocephalus:
▢ Idiopathic intracranial hypertension:
▢ Head injury:
DISORDERS OF CEREBELLAR FUNCTION
DISORDERS OF THE SPINE AND SPINAL CORD
▢ Cervical spondylosis:
▢ Lumbar spondylosis:
▢ Spinal cord compression:
▢ Intrinsic diseases of the spinal cord:
DISEASES OF PERIPHERAL NERVES
▢ Entrapment neuropathy:
▢ Multifocal neuropathy:
▢ Polyneuropathy:
▢ Guillain–Barré syndrome:
▢ Chronic polyneuropathy:
▢ Brachial plexopathy:
▢ Lumbosacral plexopathy:
▢ Spinal root lesions:
DISEASES OF THE NEUROMUSCULAR JUNCTION
▢ Common things between Myasthenia Gravis and Lambert-Eaton myasthenic gravis:
Both presents with painless weakness of muscle
Both are autoimmune disease
Both of them have autoantibodies present in circulation
Both affect Neuromuscular junction
▢ Differences between Myasthenia Gravis and Lambert-Eaton myasthenic gravis:
Myasthenia gravis
Lambert-Eaton myasthenic gravis
Pathogenesis
Antibodies directed against Acetylcholine receptor in the post-junctional membrane of the neuromuscular junction -> Complement-mediated inflammatory responses -> Reduces the number of acetylcholine receptors -> Damages the end-plate
Other autoantibodies against Muscle-specific kinase (MuSK) which is involved in the regulation adn maintenance of acetylchoine receptors.
Antibodies directed against Voltage-gated calcium channel
C/F
Muscle weakness
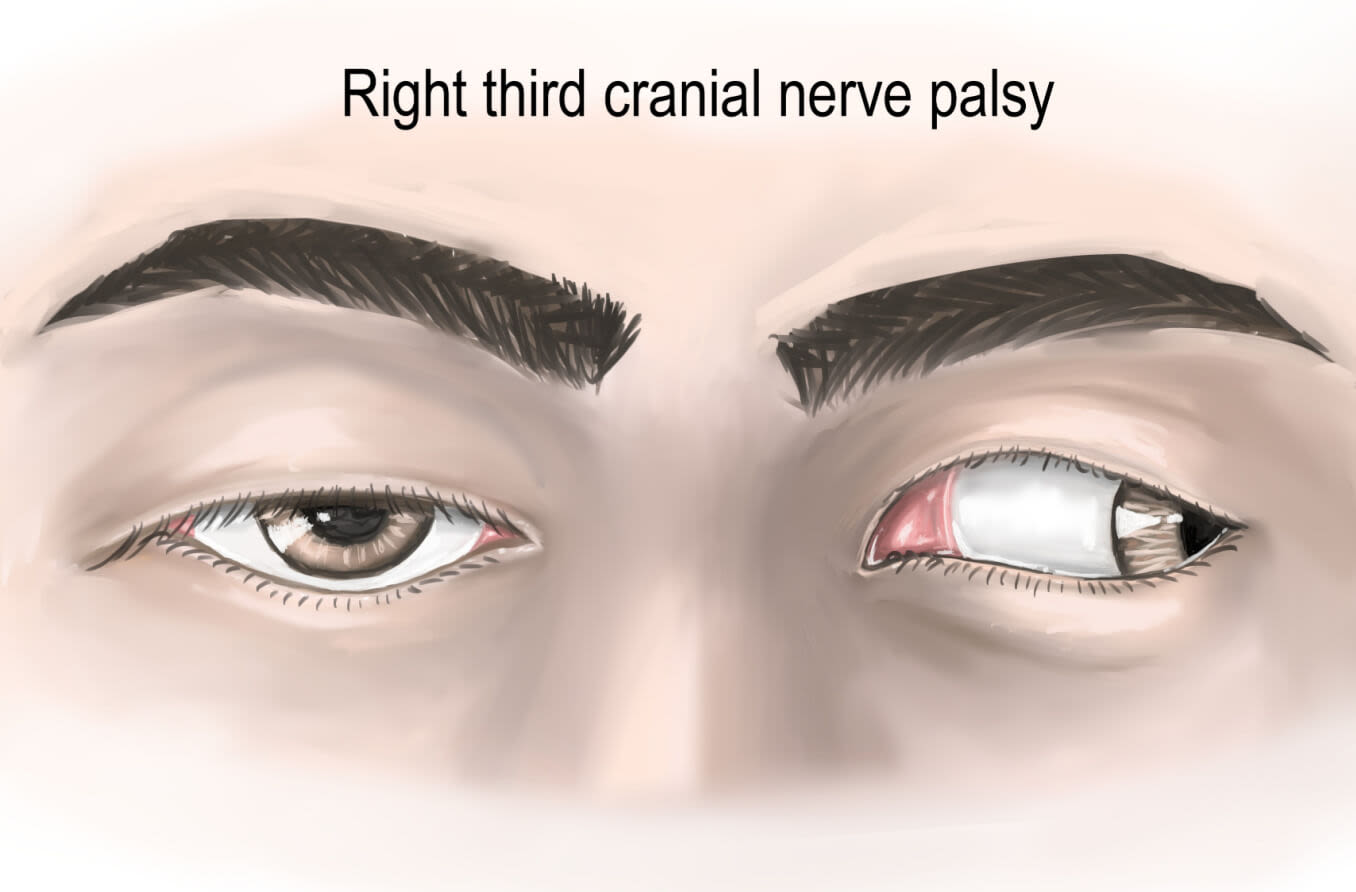
Intermittent ptosis or Diplopia -> Oculomotor muscle weakness
Weakness of Chewing
Swallowing
Speaking
Limb muscles -> Limb movement difficulty
Respiratory muscles -> Respiration failure
Ineffective cough -> Aspiration
Progressive
Cogan's lid twitch sign
Thymoma (15%) or Thymic follicular hyperplasia
Organ-specific autoimmune diseases
Exacerbating drugs
Penicillamine
Aminoglycosides
Quinolones
Investiagion
Tensilon test (IV injection of the short-acting anticholinesterase Edrophonium bromide)